Colour Vision Testing Guide for EASA pilots
- Jordan Penning

- Apr 11, 2021
- 11 min read
Updated: Apr 28, 2021
By Jordan Penning







A number of questions go through your mind if you fail the Ishihara at a class 1 medical. What secondary tests are available? Which test is the best? Where can I do the test? How many tests can I take? What happens if I fail?
This article is designed to aid your decision making, helping you to understand the secondary tests in more detail and give you the information you need to make the right decisions.
Introduction
ICAO sets the worlds medical regulations and implementing rules that EASA uses. The current regulation requires that pilots must have ‘the ability to perceive readily those colours necessary for the safe performance of duties.’ (Manual of Civil Aviation Medicine, 2012)
Clinical tests used by NAAs(National Aviation Authorities) have been designed to detect the presence and severity of colour deficiencies in a respondent, however no clinical test yet provides a measure of the effect on operating an aircraft. (Defence Technology Agency, 2015) However some argue that this is not needed if an accurate result of the severity of colour vision loss can be shown, this can then be used as a judgment itself on the respondent’s ability to perform. (CAA,2006) (CAA, 2009)
This could be perceived though as a stigma or lack of education related to colour vision as there is no evidence to suggest that CVD will affect the respondent’s ability to perform safely, reiterated by the ICAO Manual. (Defence Technology Agency, 2015). Pass marks vary between NAAs, this creates difficulty and confusion, as a candidate in one state may be issued a commercial medical and in another authority be denied. (Watson, D., 2014)
There are a large variety of testing options for colour vision; from Lanterns, Anomaloscopes, colour matching or sequencing and computer tests, all of which are lab-based tests. This is the means by which NAAs determine whether someone is colour safe for his/her positions as a pilot. However, as they are lab-based test, they don't truly represent the cockpit environment and thus can not definitively state whether someone is safe to fly an aircraft, there are many cases whereby a candidate has failed all lab-based colour vision testing but is perfectly safe to fly an aircraft, demonstrated through the use of practical real-world aviation colour vision testing.
Furthermore, the CMO of Australia had recently released a statement in February 2020 which reinforces this. '
‘Research in recent years has shown relying on diagnostic tests alone may be unnecessarily limiting when considering the impact of colour vision deficiency on aviation safety. Advances in technology, operating techniques and human factors training can now mitigate many of the safety risks of colour vision deficiency. Technology to assist pilots has developed significantly and the impact of colour vision deficiency on aviation safety should take these changes into account. These factors have been recognised overseas, most recently in New Zealand where a new approach to colour vision deficiency came into effect in May 2019, which includes an operational colour vision assessment.’ (The CASA Briefing - February 2020, 2020)
Therefore some ICAO states have implemented practical flying tests for colour vision, named the OCVA/OCVT. This is currently the fairest way to test a pilot CVD.
What secondary tests are available in EASA?
Currently in the EASA regulation MED B.075 there are 3 tests accepted for proving that you are colour safe for the issue of an unrestricted class 1 medical. However, some individual EASA states may choose to accept only certain types of tests. This can be found either on the authorities website or by contacting them. This is frustrating as it means there isn't consistency in testing methods across Europe and can lead to someone being rejected in one state and accept in another. But the majority of EASA states do accept all three testing methods for colour vision below.
Lantern testing: There are three types of lantern tests within the EASA regulation. The Holmes Wright, Beyne and the Spectrolux. Each type of lantern test varies, using different colour variants and a number of lights. However, all three tests have the same luminance you would see in aviation; the brightness of the lights varies to give the hardest possible viewing task to replicate bad weather and maximum distance. These lantern tests do not test for blue-yellow (Tritan) defects, cannot be used to identify the type of CVD or quantify severity. The HW(A), Beyne and Spectrolux lanterns will fail protanopes, while passing some anomalous trichromats (protan and deutan). The Beyne and Spectrolux lanterns differ from the HW(A), in that they will also fail significant numbers of CVN subjects. (K. G. H. Bailey, T. Carter, 2016)
Holmes Wright Lantern
The most common lantern test is the Holmes Wright Lantern A. There were originally two versions, A and B. A was specifically designed for aviation, with the B version designed for maritime. (Birch J., Roden M, 1993)

The HWL has been validated since the 1970s and is very good in passing only candidates with a mild colour deficiency that can perform the important safety tasks and passing 100% of colour normal’s. The test consists of 9 pairs of lights, displaying either Red, Green or White. The candidate has to correctly name all 9 pairs to pass the test. First, the test is conducted in Mesopic light conditions (Dusk), if the first run is failed a 2nd and 3rd run is taken. If there are any errors in the 2nd and 3rd run, the test is then taken in Dark conditions. If the candidate passes this final run of 9 pairs they will pass the test.
Beyen Lantern
The next most popular lantern test in Europe is the Beyne.

The device is made by the manufacturer Luneau France with the name Tritest L3. Another name for the device or the test procedure is Beyne Type 2 (Aviation). The device is no longer in production. The production period of the test device at DLR is around the 1980s. The first devices of this type were produced by another manufacturer as early as 1951 and are known as the "original Beyne Lantern".
Unlike the HWL, the Beyne only displays 1 light at a time, it also has 5 different colours.
This is only conducted in Mescopic light conditions,
2 testing protocols (red, green, blue, yellow-orange and off-white)
1 second per colour with 3 minutes of arc aperture
1 s / 3’ x 3 presentations (pass if no error on 2 of 3 presentations)
Again no errors are allowed, in order to pass the test. This test was popular in France, Italy and is still used in a number of EASA states.
Spectrolux
The final lantern test and the least common across Europe is the Spectrolux.

The Spectrolux lantern made in Switzerland came into service in the 1980s for use in aviation and displays 12 pairs of red, green, and white signal lights that have the same chromaticities as airport navigation lights. (Color Vision Tests for Aviation: Comparison of the Anomaloscope and Three Lantern Types 2005)
No errors can be made during the test, it is also conducted in light conditions, which differs from the HWL and Beyne.
The Spectrolux lantern has twelve vertical pairs of combinations of red, green, or white lights, with two different intensities and hue of each colour. A total of 2 runs of the 12 pairs are carried out in the same order each time, and every colour had to be named correctly (as ’red,’ ’green,’ or ’white’) to pass. No demonstration of colours prior to the test is given, but subjects are advised of the colours they could expect.
Figure 8 shows a comparison between each of the EASA Lantern tests.

(Color Vision Tests for Aviation: Comparison of the Anomaloscope and Three Lantern Types 2005)
Anomaloscope testing:

Generally recognised as the gold standard and the best instrument for differentiation of normal trichromats from individuals with red/green colour deficiencies, for differentiation of protan and deutan types amongst the red/green deficient and also recommended for diagnosis and differentiation of the level of deficiency. (Procedures for testing colour vision, 1981)
Like the lanterns, there is several different version of this test, from the Nagel, pictured above. This is a manual Anomaloscope meaning there is no computer software. There is also the HMC Anomalscope which is a computerized test. The Nagel and HMC are the most popular and follow the same principles in testing.
This test is based on colour matching where the respondent views a disk split into two half fields as shown in the picture above, through the device telescope.

The scoring of this test is much more complicated than the lanterns, it is explained below.
The respondents need to match the two half fields in both colour and brightness by changing the red/green mixture at the top disk and the brightness of the yellow field at the bottom disk using the two knobs located on the side of the machine. The matches are recorded on a scale and put into a graph. The score is shown in two items, the range of matches and the mid-point. The range of results can be from 0-73. Normal trichromats achieve a match average consistent to a mid-scale range of settings 36 to 44 , with 40 being the normal midpoint. When the results are outside the normal trichromatic range, the midpoint and the extent of the range will be used to determine the type of colour deficiency and its severity. (Ncbi.nlm.nih.gov., 1981)

The graph above shows how the testing is recorded and how the matching range determines a person type of CVD and severity. To pass the test according to the EASA regulations, the matching range has to be 4 scale units or less and be trichromatic. This basically means you must have 3 cones, either Deutanomally, Protanomaly or Normal. A matching range lower than 30 shows a Detuan deficiency (green) and above 45 shows a Protan deficiency (red). The matching range has to be a maximum of 4 units difference, for example, 22-26 would be a pass, but 22-27 would fail. On this graph, you can see the passes represented by the blue diamonds. The top and bottom of the graph show people who aren't trichromats, have lost one cone and have the largest matching range. DA stands for Deutan whilst PA stands for Protan.
However whilst EASA states accept a trichromatic result with 4 SU or less, meaning Detuan or Protan with a matching range of 4 units or less. The UK CAA have a different regulation which states 'This test is considered passed if the colour match shows normal trichromacy, i.e. a matching midpoint of 38-42 scale units and the matching range is 4 scale units or less;'. This meaning the person must have a normal colour vision to pass under the new UK CAA regulation.
CAD testing:
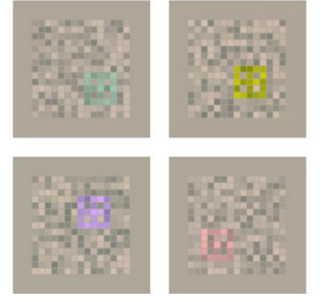
The test lasts 15 minutes in which a colour square will move to one of four corners against a grey pixel background simulating camouflage technique, the candidate must then press a button to which of the four corners he or she believes the coloured square moved to. When the button is pressed the next coloured square will be displayed. The test progressively gets harder with the colour fading against the grey background, even for colour normals. The computer programme works out a score that relates to the respondent’s colour vision. The test is normally taken in a dark condition with a monitor that is automatically calibrated. (Cityoccupational.co.uk, 2012) (CAA, 2009)
The UK CAA then determined the safe colour vision loss level, 6 SU (Standard units) for Deutans and 12 SU for Protans. (CAA, 2009) A respondent must get a score equal to or lower to pass the test depending on what type of colour deficiency they have. This pass mark developed from the City University’s PAPI light test was created to relate the pass mark of the CAD to the most safety-critical task. The idea is that if a respondent can pass the CAD, they could definitely see the PAPI lights.
The DTA 2015 report explains there are ‘Four aspects of the validation process are however open to challenge.
The University PAPI simulator was not representative of the colour or intensity of real PAPI lights. Rather the University PAPI simulator modified the colours of the signal lights to exploit lines of colour confusion.
City University eliminated the secondary intensity cue that is designed into the real PAPI.
Thirdly, simulator lights were only presented for 2-3 seconds, after which the subject was required to state how many red lights had been shown. By comparison, the real PAPIs are continuously visible to the observer when interpreting the signal.
Finally, the pass mark in the CAD test was adjusted so as to be conservative. A proportion of respondents who were able to read the city University PAPI simulator without error, fall below the prescribed CAD pass mark.
As such the CAD test applies four levels of conservatism with result in a significant proportion of CVD respondents being excluded’. (Defence Technology Agency, 2015) Furthermore, concerns regarding the CAD test stems from that it is based on the PAPI. It is pointed out in the submissions that not all airfields have PAPI; it is a redundant aid that is prone to errors, and it is not a requirement for a safe landing. (CVDPA, 2017) (Caa.govt.nz, 2015)
It is also important to note that the maker of the CAD himself Dr John Babur in the Australian appeal tribunal said “The CAD system wasn’t designed specifically for aviation. It was designed for assessing colour vision.” “…the CAD test was not intended in any way to use direct information on operational tasks.” “…that does not make the CAD an operational test.” (O’Brien and Civil Aviation Safety Authority, 2015)
CVDPA have shown a video clip of a CAD test (where Dr Pape was the test subject) to a significant number of highly experienced pilots. Without exception, the response has been that the test resembles nothing any pilot has ever encountered in either normal or abnormal operations in any type of aircraft. The CVDPA stated ‘this test does not simulate any operational action or situation.’ (CVDPA, 2017) (Pape, A, 2015)
The pass criteria for the CAD appears to be arbitrarily raised when compared to the pass criteria for the PAPI simulator. (DTA Report 405, 2015)
Research conducted by City University and the CAA was not subject to any independent review. ‘The CAA 2006 and 2009 studies were conducted under contract to the CAA by the City University of London and subsequently published by the CAA’.
Which is the best for testing colour vision?
The problem with all these tests is they are lab-based, they cannot determine whether someone is safe to fly an aircraft.
So the best test is actually the OCVA, this is not currently an EASA testing method but is used by CASA and the NZ CAA. The OCVA is a practical real-world flight test to determine you can safely fly an aircraft, it is also recommended that a person has some flying experience to understand the basic of controlling an aircraft.
More on the OCVA will be in our next article so make sure to sign up for a free account with ECDAA here: https://www.ecdaa.com/join-now to get a notification when this article comes out.
How many tests do I need to pass?
Only one test needs to be passed. In the EASA regulations, as soon as you pass one of the tests in the list you are classed as colour safe.
What happens if I can't pass the tests?
If you cant pass any of the tests, the best thing to do is to look at where there is an OCVA or a similar type of practical flight tests. Try and get a medical with the authority that has the OCVA or similar test. It may be worth also telling your current authority that you have passed the OCVA as proof you can safely fly an aircraft.
Join ECDAA in helping us to achieve implementing the OCVA or a similar test across Europe.
Conclusion
If you liked this and want to find out more information on testing and regulations as well as the critical analysis of the current UK colour vision regulation, you can access my research here: https://www.ecdaa.com/useful-resources-1
References
Bailey, K. and Carter, T. (2016). Consistency of secondary colour vision tests in transport industries. Occupational Medicine, 66(4), pp.268-275. Available at: https://academic.oup.com/occmed/article/66/4/268/1752619 (Accessed 9 May 2019)
CAA, (2006). CAA Minimum Colour Vision Requirements For Professional Flight Crew - Part 1. CAA. Available at: (Accessed 19 March 2020).
CAA, (2009). CAA Paper 2009/04 Minimum Colour Vision Requirements For Professional Flight Crew. CAA. Available at: (Accessed 19 March 2020).
City-occupational.co.uk. (2012). Research. Available at: http://www.city-occupational.co.uk/research/ (Accessed 5 May 2019).
Civil Aviation Safety Authority. (2020). The CASA Briefing - February 2020. Available at: https://www.casa.gov.au/publications-and-resources/publication/casa-briefing-february-2020 (Accessed 8 March. 2020).
Color Vision Tests for Aviation: Comparison of the Anomaloscope and Three Lantern Types. (2005). Aviation, Space, and Environmental Medicine. Available at: http://peter2000.co.uk/aviation/misc/JAR_colour_study.pdf (Accessed 3 May 2019)
CVDPA (2010). A CVD Pilot’s Perspective. Available at: http://cvdpa.com/images/pdf/1.%20CVDPA%20Presentation%20to%20Shane%20Carmody%20- %2010-03-17.pdf (Accessed 8 March. 2020). • CVDPA (2017). Submission by the Colour Vision Defective Pilots Association (CVDPA). CASA Medical Certification Standards Discussion Paper. CVDPA. Available at: http://cvdpa.com/images/pdf/CVDPA%20Submission%20to%20AvMed%20Discussion%20Paper.pdf (Accessed 8 March. 2020).
Defence Research and Development Canada (2017). Assessment of the Next Generation of Colour Vision Tests for Pilots and Aircrew. Waterloo. Available at: https://cradpdf.drdcrddc.gc.ca/PDFS/unc286/p805813_A1b.pdf (Accessed 8 March. 2020).
Defence Technology Agency. (2015). Colour Vision Requirements For Aircrew. Auckland 0744 New Zealand: Defence Technology Agency. Available at: https://www.cvdpa.com/images/further_reading/articles/DTA%20CVD%20Report%20- %20Ryan%20Brookes.pdf (Accessed 19 March 2020).
K. G. H. Bailey, T. Carter, Consistency of secondary colour vision tests in transport industries, Occupational Medicine, Volume 66, Issue 4, June 2016, Pages 268–275,
Manual of Civil Aviation Medicine. (2012). 3rd ed. ICAO. Available at: https://www.icao.int/safety/aviation-medicine/Documents/8984_cons_en.pdf (Accessed 1 May 2019).
Ncbi.nlm.nih.gov. (1981). COLOR VISION TESTS. Available at: https://www.ncbi.nlm.nih.gov/books/NBK217823/ (Accessed 3 May 2019).
O’Brien and Civil Aviation Safety Authority (2015) AATA 93 (AATA). Available at: pp. https://www.cvdpa.com/images/pdf/aat-decision-2015-02.pdf. (Accessed 8 March. 2020).
Pape, A. (2015) The Colour Assessment & Diagnosis (CAD) Test: An ‘Ishihara Test’ by another name? ASAM Annual Scientific Meeting, Adelaide. Available at: https://www.cvdpa.com/images/further_reading/presentations/ASAM%202015%20Pape%20Final.pdf (Accessed 8 March. 2020).
Watson, D., (2014). Aviation, Space, And Environmental Medicine, Volume 85, Number 2. 85th ed. Aerospace Medical Association, pp.pp. 148-159(12)



Comments